Download here. You can study at your leisure abstracts of the presentations at this summer's smoking cessation trade fair – most of them, that is, except the one for the presentation by public health minister Anne Milton, which was not available at the time of going to press (see p. 50).
The subject areas are harm reduction; prisons, probation and mental health; payment by results; campaigns; tactics of the tobacco industry.
In the middle of the brochure there is (as one might expect) a helpful section called 'Information from our sponsors', starting with a full page of 'information' about Champix, followed by 'information' about other kinds of smoking cessation medications (can double your chance to quit), followed by 'information' about a helpful organisation called the National Centre for Smoking Cessation and Training, which does pretty much what it says on the tin. Out there in the real world we could call this 'information' advertising, indicating the clear possibility of a commercial interest in the success of the conference, but we wouldn't want anyone to think that the pharmaceutical interests in question had anything to gain from government-endorsed smoking cessation campaigns, surely? (shhh, don't tell the World Health Organisation!)
Thursday, 30 June 2011
New Zealand prison ban begins
Spare a thought for prisoners in New Zealand who face a smoking ban from 1 July (already active as they are 12 hours ahead). Some trouble is expected including disturbances and the possible smoking of tea leaves and nicotine patches.
I find it very hard to see a need for this. Actually impossible.
I find it very hard to see a need for this. Actually impossible.
BBC coverage of Save our Pubs
I suppose it was as much as we could expect from the BBC. It reports on a Cross-Party group that wants to see an amendment to the smoking ban.
Andrew Neil reading from a Department of Health briefing as if it were a credible source of facts, and a list of what has damaged the licensed trade other than the smoking ban, more or less claiming that pubs have their day and the smoking ban is irrelevant. John Hemming arguing for a change principally to stop the mess and inconvenience of going through groups of smokers on the way in and out of the pub. Hilary Benn MP apparently oblivious to the pubs throughout the country that don't have gardens (is he still Labour?).
Nothing to challenge the underlying justification for the ban ... only arguments along the lines of 'the ban is very well meaning but not very well thought out'. And the only convert on the issue, Nick Herbert MP (Conservative), who has decided that the health of bar staff might cause him to rethink his opposition to the ban, should another opportunity arise to vote on the issue. And it won't, of course.
Thanks, Aunty Beeb.
Andrew Neil reading from a Department of Health briefing as if it were a credible source of facts, and a list of what has damaged the licensed trade other than the smoking ban, more or less claiming that pubs have their day and the smoking ban is irrelevant. John Hemming arguing for a change principally to stop the mess and inconvenience of going through groups of smokers on the way in and out of the pub. Hilary Benn MP apparently oblivious to the pubs throughout the country that don't have gardens (is he still Labour?).
Nothing to challenge the underlying justification for the ban ... only arguments along the lines of 'the ban is very well meaning but not very well thought out'. And the only convert on the issue, Nick Herbert MP (Conservative), who has decided that the health of bar staff might cause him to rethink his opposition to the ban, should another opportunity arise to vote on the issue. And it won't, of course.
Thanks, Aunty Beeb.
Amend smoking ban reception, London, 29 June 2011
First account of reception held at Westminster yesterday for Save our Pubs & Clubs campaign. More will follow.
| Admit One |
Wednesday, 29 June 2011
Further BMA demand to ban smoking in cars
The BMA wants us to stop smoking in cars.
How can a BMA official talk about smoke levels in 'a car', 'a house', or 'a pub', and expect to have these units of measurement taken seriously?
And does he really believe that breathing in the product of an exhaust pipe is safer than inhaling secondary smoke? Why does he qualify this by saying 'in terms of particulate matter released' – because of the gaseous content of exhaust fumes, which don't lend themselves to particulate measurement?
Michael McFadden's contribution to the argument about toxicity of cigarette fumes (including its toxicity in relation to that of exhaust fumes) has featured in an earlier blog post. He points to serious flaws in studies on smoke inhalation.
We don't need a ban on smoking in cars.
London-based Dr Noble said: “In cars, particle concentrations are 27 times higher than in a smoker’s home and 20 times higher than in a pub, in the days when you could smoke in public places.
“It would be safer to have your exhaust pipe on the inside of your car than smoke cigarettes in terms of fine particular matter released.There is probably a good reason why neither Dr Noble nor anyone else from the BMA made a name for themselves by insisting that smoking bans in homes and cars should take priority over smoking bans in adult recreational venues. They could have saved millions of young children from up to five or six years of perilous exposure to secondary smoke. Why has no one sued them?
How can a BMA official talk about smoke levels in 'a car', 'a house', or 'a pub', and expect to have these units of measurement taken seriously?
And does he really believe that breathing in the product of an exhaust pipe is safer than inhaling secondary smoke? Why does he qualify this by saying 'in terms of particulate matter released' – because of the gaseous content of exhaust fumes, which don't lend themselves to particulate measurement?
Michael McFadden's contribution to the argument about toxicity of cigarette fumes (including its toxicity in relation to that of exhaust fumes) has featured in an earlier blog post. He points to serious flaws in studies on smoke inhalation.
We don't need a ban on smoking in cars.
European Union doubts about plain packaging and an Aussie caricature
Further to criticism from other quarters, the European Union has added its voice to the doubts being expressed about the legitimacy of the plain packaging strategy, the World Trade Organisation fearing that it breaches laws on intellectual property. The Australian government is convinced it has done its homework and insists it can work the legislation within intellectual property rights law. The reporter clearly has reservations:
The Health Minister refused to answer questions about the size of the legal budget the government has set aside to cover the cost of challenges brought by the tobacco industry. When asked whether lawyers would be the biggest winners out of plain packaging laws, Ms Roxon said: "I think the public stand to be the biggest winners out of this measure."Meanwhile writer David Campbell shows the caricature that results when the media decides not to take both sides of an issue seriously.
Today, Save our Pubs and Clubs Campaign goes to Westminster
BBC report here, and This is Bristol here. A reception will be held at Westminster today for the campaign to amend the smoking ban, involving three MPs, Forest, publicans and others. It will send a message that many, many people are not happy with the comprehensive smoking ban and see no reason that smokers must have nowhere to socialise except in their own homes.
Asking for permission to set up smoking rooms is a risky strategy as it concedes that secondary smoking is itself a specific problem that requires a legislative solution. The only legislative solution required is regulated indoor air quality standards. dealing not only with cigarette smoke but with all air-borne pollutants. No legislation is required to regulate where people may smoke in business establishments, or whether staff may enter specific areas to carry out their duties. The air must be cleared free of toxins, so that people can work anywhere.
Freedom to Choose (Scotland) supports the campaign to amend the ban, but would prefer the approach offered here. Still, it is magnificent to see growing opposition to the smoking ban – I look forward to hearing more reports of the day.
Asking for permission to set up smoking rooms is a risky strategy as it concedes that secondary smoking is itself a specific problem that requires a legislative solution. The only legislative solution required is regulated indoor air quality standards. dealing not only with cigarette smoke but with all air-borne pollutants. No legislation is required to regulate where people may smoke in business establishments, or whether staff may enter specific areas to carry out their duties. The air must be cleared free of toxins, so that people can work anywhere.
Freedom to Choose (Scotland) supports the campaign to amend the ban, but would prefer the approach offered here. Still, it is magnificent to see growing opposition to the smoking ban – I look forward to hearing more reports of the day.
Liberal Vision revisited, again
This time, a discussion of the relevance of libertarianism to the smoking ban, for the benefit of people who think of themselves as libertarian but still believe that the issue is about dirty air caused by smoking ('The right to swing my fist ends where the other man’s nose begins'), rather than an invasion of personal autonomy, and the right of individuals and businesses to decide their own rules of engagement.
I haven't considered the issue of libertarianism enough to know whether I am a libertarian. But you don' t have to be a libertarian to realise that the only way the health authorities have got away with the smoking ban so far has been by convincing enough people that secondary smoke is a killer (even though there is no evidence to support the hypothesis that isn't distorted by compounding factors). And to convince people of something so unlikely, they must have been distorting the truth for some ulterior motive – which is not acceptable to me and many readers of blogs like this one. Government needs to be reliable, truthful and keep things in proportion. It fails on all counts with this legislation.
I haven't considered the issue of libertarianism enough to know whether I am a libertarian. But you don' t have to be a libertarian to realise that the only way the health authorities have got away with the smoking ban so far has been by convincing enough people that secondary smoke is a killer (even though there is no evidence to support the hypothesis that isn't distorted by compounding factors). And to convince people of something so unlikely, they must have been distorting the truth for some ulterior motive – which is not acceptable to me and many readers of blogs like this one. Government needs to be reliable, truthful and keep things in proportion. It fails on all counts with this legislation.
Monday, 27 June 2011
Cabin crew more at risk from AIDS and air accidents than cancer, says study
From Lifestyle Reviews – a 2002 study shows that cabin crew studied in Germany between 1960 and 1997 died more frequently from accidents and from acquired immunodeficiency syndrome than from many types of lung cancer and that 'occupational hazards seem not to contribute strongly to the mortality of airline cabin attendants'. Lung cancer incidence was low, even though exposure to SHS occurred commonly in aircraft until the mid-1990s.
Male and female data shown.
Aeroplanes are fertile environments for cross-infection.Thoroughly ventilating aircraft is imperative for maintaining air quality – smoke, as anywhere, constitutes a minor pollutant.
Male and female data shown.
Aeroplanes are fertile environments for cross-infection.Thoroughly ventilating aircraft is imperative for maintaining air quality – smoke, as anywhere, constitutes a minor pollutant.
Sunday, 26 June 2011
Tobacco control aims to lead global fight against non-communicable diseases, claims evidence base of success
The World Lung Foundation, an advocacy group that endorses tobacco control, looks forward to the forthcoming global summit on non-communicative diseases (article from the European Society for Medical Oncology, or ESMO). This summit aims to consolidate further the aims of tobacco control, taking the rest of the agenda on tackling non-communicative diseases in its wake. An agenda proposed by the NCD Alliance in the Lancet proposes the following 'priority interventions', which are 'tobacco control, salt reduction, improved diets and physical activity, reduction in hazardous alcohol intake, and essential drugs and technologies' and a goal of a smoke-free world by 2040.
Is it not rather startling to find interventions in lifestyle factors at the heart of every one of these first five priorities except the one on drug development?
Discussing the events of a UN meeting earlier this week, Stephen Hamill of the World Lung Foundation says:
On the basis of this 'success', civil society groups (whatever they are) now want more tobacco control on the agenda, including more steps taken to implement the FCTC.
Who knows what will come out of the forthcoming summit on non-communicable diseases next September, but it would appear that one result will be more commitments made by countries under pressure from international organisations that will bedevil democratic accountability to their electorates. This will effect laws on food content and alcohol regulation as well as tobacco. Policing global public health, with other environmental and genetic factors in ill health pushed down the priority list, promises to be a huge diversion of resources from vital health issues.
Is it not rather startling to find interventions in lifestyle factors at the heart of every one of these first five priorities except the one on drug development?
Discussing the events of a UN meeting earlier this week, Stephen Hamill of the World Lung Foundation says:
With so many issues on the table, there was a call to identify and prioritize cost-effective interventions with an evidence base of success. Tobacco control meets this criteria. Implementing the Framework Convention on Tobacco Control (FCTC), the world's only public health treaty, would save hundreds of millions of lives at very little cost. We heard numerous civil society groups testify that to combat NCDs, the UN Summit must accelerate implementation of the FCTC. As advocates, however, we should take nothing for granted, and we have hard work ahead to ensure that this remains an outcome of the Summit. [emphasis added]What evidence base of success would that be? Smoking cessation rates are nothing to boast of. Evidence to support the tobacco display ban was 'inconclusive' (Christine Graham at col 19996). Arguments continue about the evidence that plain packaging will make any difference. A big fairy tale about a drop in heart attack admissions was used to boost the popularity of the smoking ban in Scotland, and elsewhere. Yet we are told that tobacco control has an evidence base of success. That looks like material for FOI if ever I saw it, but no doubt the World Lung Foundation is under no obligation to reveal anything.
On the basis of this 'success', civil society groups (whatever they are) now want more tobacco control on the agenda, including more steps taken to implement the FCTC.
Who knows what will come out of the forthcoming summit on non-communicable diseases next September, but it would appear that one result will be more commitments made by countries under pressure from international organisations that will bedevil democratic accountability to their electorates. This will effect laws on food content and alcohol regulation as well as tobacco. Policing global public health, with other environmental and genetic factors in ill health pushed down the priority list, promises to be a huge diversion of resources from vital health issues.
Friday, 24 June 2011
ASH Scotland: Assaulting smokers with bilge about third-hand smoke
The anti-smoking professionals are getting a bad press this week, but this gets even worse.
A briefing called Third-hand Smoke has appeared today. It was only a matter of time as ASH Scotland has been gathering information on Third-hand Smoke for some months now. The opening is classic ASH Scotland:
A further purpose is to continue pushing ASH Scotland's agenda to get people smoking outside. ASH Scotland's strategy document Beyond Smoke-free includes the following in its short-term aims:
A briefing called Third-hand Smoke has appeared today. It was only a matter of time as ASH Scotland has been gathering information on Third-hand Smoke for some months now. The opening is classic ASH Scotland:
- the ‘three r’ definition of third-hand smoke is that it describes residual tobacco smoke pollutants which remain on surfaces and in dust after tobacco has been smoked, are re-emitted back into the gas phase, or react with oxidants and other compounds in the environment to yield secondary pollutants
- even without understanding what third-hand smoke is, people have long been aware of its presence and are beginning to understand how it can affect clothes, hair, cars and homes, and create stains and odours
- existing evidence on THS suggests a strong need for further research to close gaps in the current understanding of the chemistry, exposure, toxicology, and health effects, as well as behavioural, economic, and socio-cultural consequences
- whereas there is a long-established evidence base for the health impact of second-hand smoke, there is still a lack of human health studies on the potential health impact of third-hand smoke
- the greater and more quantifiable health dangers from SHS suggest that health professionals should focus on reducing exposure to SHS, including by promoting smoke-free homes and vehicles. [italic emphasis added]
In other words, 'people know that smoke is smelly and stains things over time, but we haven't be able to demonstrate any health effects in the literature yet. We can still carry on pestering you about secondary smoke though.' Well, that was worth a shed-load of taxpayers' money. Curiously, it then goes on to explain that residual smoke reacts with oxides and other chemicals including nitrous acid, which is 'produced in engine exhaust emissions but is also a common indoor pollutant produced by poorly vented domestic gas appliances'. Wouldn't it be better to maintain regular checks on these gas appliances than to mess about warning people on third-hand smoke, which they don't even know is dangerous? Researchers have so far failed to find harmful doses of any substances in third-hand smoke even when increasing nitrous acid concentrations to levels much higher than normal. But that won't stop belief in the concept. One respondent even cites third-hand smoke as a reason to ban electronic cigarettes.
The third-hand smoke briefing from ASH Scotland shows limited understanding of second-hand smoke too. In one sentence to describe second-hand smoke it says: 'Research demonstrates that tobacco smoke is a toxic substance with no safe level of exposure, and that the risks from exposure are largely dose-related' [emphasis added]. If it's dose related, why won't a tiny little dose cause negligible damage? (oh, dear!)
This third-hand smoke concept is insidious. It fits so well with the denormalisation of smokers. Having removed smoking from the public sphere, it now follows them to the private sphere. Question – What could be the intention of this kind of statement?:
A 2010 study* indicated that third-hand smoke accumulates in smokers' homes and persists even after homes have been vacant for two months and are cleaned and prepared for new residents; the study suggested that non-smokers living in former smoker homes are exposed to THS in dust and on surfaces. (* Matt, George E et al. When smokers move out and non-smokers move in: residential thirdhand smoke pollution and exposure. Tobacco Control, 2011;20:e1. http://tobaccocontrol.bmj.com [Accessed 06 May 2011])Answer – to devalue the effects of smokers: the properties they own, or rent. To impoverish them, basically. And to devalue smokers as buyers of property and (especially) as tenants. Note that this study emerged in 2010, and they still, half-way through 2011, don't have any evidence that third-hand smoke harms anyone. Yet they are printing this rather inflammatory material It talks of a potential health hazard to infants: no sick babies to hand, just potential research contracts.
A further purpose is to continue pushing ASH Scotland's agenda to get people smoking outside. ASH Scotland's strategy document Beyond Smoke-free includes the following in its short-term aims:
We must develop robust intermediate and endpoint targets to reduce second-hand smoke exposure in the home and in vehicles, in order to support awareness raising work and work in communities.And the following in its medium-term aims:
We need to be realistic about the difficulties some people have. We must promote effective harm reduction strategies, including the use of nicotine replacement for temporary abstinence, to protect children from exposure to secondhand smoke in the home.All the more easy for them, if they can persuade enough people of the dangers of third-hand smoke without needing to prove it or even show any understanding of it. The briefing does say that the research on third-hand smoke is not conclusive. But it is 'aimed at parents and carers', talks about infants crawling across the carpet and generally attempts to stir the shit on the basis of lucrative speculation, in pursuance of its agenda.
FDA goes photoshopping
TBY has covered this story, and supplied the graphics.
But consider the irony. Accepting money from interest groups is reprehensible ... until They do it. Embellishing the truth is reprehensible ... until They do it – at which times it becomes a positive duty and an artistic way to get their essential message across. Writer Charlie Hurt concludes:
But consider the irony. Accepting money from interest groups is reprehensible ... until They do it. Embellishing the truth is reprehensible ... until They do it – at which times it becomes a positive duty and an artistic way to get their essential message across. Writer Charlie Hurt concludes:
Visually, in terms of repulsiveness, there is little difference between the tactics of the abortion protesters and those of the federal government. In fact, the only difference is that the government doctored its pictures.
And you paid for them.
Revisiting Liberal Vision ...
And why not – some big names from Tobacco Control have done so ... (see comments)
Thursday, 23 June 2011
Guest post from Ohio: Creating Foundations to Move Their Ideals...and Products
The New Corporate American Business Model
Creating Foundations to Move Their Ideals ... and Products
By Pam Parker, Opponents of Ohio Bans, with permission.
There's a new and dangerous business strategy being employed in the United States. Corporations are creating Foundations who give grants to non-profits who push for laws that move their products. One thing the corporations, foundations and non-profits all share is profitability. One such corporation is Johnson and Johnson. Those who share in the profits are their partners.
The Robert Wood Foundation was created by the founder of Johnson and Johnson with over ten millions shares of Johnson and Johnson (J&J stock [i]). In 1972, it was established as a national foundation worth $1.2 billion [ii]. In 2009, the Foundation's investment portfolio increased $1 billion to $8,379,808,000 [iii]. RFJF's mission today: to help society transform itself for the better. Noble sounding, until you delve into the fact that it's what RWJF considers "for the better", foregoing what we want for ourselves or for our society. The horrifying truth is RWJF profits from what it wants for society.
The RWJF anthology "Taking on Tobacco: The Robert Wood Johnson Foundation's Assault on Smoking" publication [iv] outlines how they gave $99 million in grants to fund coalitions "housed in organisations" such as American Cancer Society (ACS), American Lung Association (ALA) and American Heart Association (AHA). This publication outlines all the organisations who received over $446 million in grants just through January, 2008. In the beginning, grants were given to organisations to promote tobacco education. Once organisations were used to receiving funding, if they did not move on to tobacco "control", their funding was cut off. The Foundation makes it perfectly clear in their publications that as a Foundation, their grant money cannot be used for lobbying. However, to quote Julia Roberts in Pretty Woman, that's just geography. It's just moving money from point A to point B while accomplishing lobbying, with smoking cessation as RWJF's ultimate goal. Over $99,000 in grant money was invested in Evaluating an Innovative Communications Campaign Designed to Increase Consumer Demand for Tobacco Dependence Treatment by Medicaid Recipients [v]. Nearly $97,000 in grant money was invested for Individual and Policy Level Influences on the Use of Various Cessation Strategies and Abstinence from Cigarettes Among Adult Smokers [vi].
RWJF points out repeatedly that coalition building is the key. Here are but a few:
- The Centre for disease Control has received grant money from RWJF [vii].
- RWJF provides funding for Tobacco Free Kids (TFK) for polls used to influence lawmakers, such as an Ohio Poll [viii] on raising cigarette taxes.
- RWJF is a major funder of the Tobacco Control Legal Consortium [ix] who helps works with communities with tobacco law-related issues such as smoke free policies (smoking bans) and tobacco control funding laws.
- Stephen Schroeder, former CEO of RWJF, returned to the University of California, San Francisco, with a $10 million RWJF grant for the Smoking Cessation Leadership Center [x].
- Glaxo Smith Klein, marketer of Nicorette, Nicoderm, Nicoderm CQ, is quoted in this article as applauding two organisations for their efforts to improve the regulation of smoking cessation aides. The two organisations, Association for the Treatment of Tobacco Use and Dependence (ATTUD) and the Society for Research on Nicotine and Tobacco (SRNT) both urged the FDA to adopt more flexible regulatory approaches to expand access to and the use of NRT products. ATTUD's FDA petition drive [xi] was funded, in part, by RWJF, SRNT is funded [xii], in part, by RWJF, Johnson and Johnson, GSK and McNeil.
- Professor Stanton Glantz, University of California, San Francisco, received grants of over $1,071,000 to create Tobacco Scam to claim smoking bans don't hurt the hospitality industry. It's been proven that most bars are hurt by smoking bans, but Glantz combines restaurants with bars (restaurants outnumber bars 5:1 while restaurant employees outnumber bar employees 10:1). (RWJF Grants 52810 and 36173). Glantz's job? To say it's all a Big Tobacco lie, and that's what his website claims [xiii]
If a group doesn't exist, the RWJF just creates and funds it. For example - Tobacco Free Kids. A brilliant marketing strategy. After all, who wouldn't want kids to be tobacco free? RWJF created and funded Tobacco Free Kids [xiv] (TFK) with $84,000000 in start up money. In 2000, TFK drafted the core principles for the World Health Organisation's Framework Convention on Tobacco Control. In fact, interveners for the Master Settlement Agreement [xv] have all received funding from RWJF, (ACS, AHA, ALA, Americans for Nonsmokers' Rights [xvi][xvii], the National African American Tobacco Prevention Network [xviii, p. 6]. The Master Settlement Agreement was originally to settle states' Medicaid lawsuits against the tobacco industry for recovery of tobacco-related health care costs [xix]. It has evolved into lobbying states to spend money on smoking cessation, quit lines and giveaways of nicotine replacement products, such as patches and gum.
For decades, RWJF has financed a felowship program, paying up to $165,000 each. This year [xx] there are six RWJF fellows, assigned free of charge to: Senator John D. Rockefeller (C), Senator Orin Hatch (R), Senator Kent Conrad (D), one is assigned to the Senate Committee on Finance, two are assigned to Health and Human Services, Office of the Secretary.
With the exception of one FDA employee and three tobacco industry representatives, every member of the newly created FDA Tobacco Products Scientific Advisory Committee has received direct funding from RWJF.
The latest (2008) Tobacco Cessation Guidelines were updated by a panel of tobacco control "experts", seventy per cent of whom directly received RWJF grants and or / awards.
Consumers are now being told that using more than one type of NRT can triple quit rates [xxi].
RWJF's funding of tobacco control all links back to smoking cessation. Why is this important? As noted in this article, Glaxo Smith Kline markets Nicorette, Nicoderm, Nicoderm QC, but these are Johnson and Johnson products, as well as Nicotrol which belongs to J&J's McNeil Company. In fact J&J has pretty much cornered the market on over the counter nicotine replacement products. The lobbying for payment of NRT, increased taxes on cigarettes, lobbying for smoking bans (excuse me, "advocating") all increase not only J&J's profits, but because RWJF owns millions of shares of J&J stock, so does RWJF profit.
Their partners also pull in a pretty penny. The ACS's IRS 990 form on-line shows that the ACS brought in over $9,009,812 in revenue from Quit Lines [xxii, p. 11]. The ACS is a Quit Line vendor. The same 990 form shows the ACS claiming $0 [xxiii, p. 12] in lobbying expenditures, yet they claim $11,662,010 in grants to others for lobbying purposes [xxiv]. Interesting how no one seems to claim money for lobbying purposes but claims to give millions and millions away to others for the others to lobby. The ACS published a report in 2003 that showed that 91.4% of former smokers quit cold turkey [xxv], yet they not only push NRT, they've been paid for the use of their logo on Nicorette, according to a 1996 US Attorney General's report. According to the report, the ACS entered into a licensing agreement in August, 1996 for annual payments of $1 millions for the use of their logo on Nicoderm CQ and Nicorette. The same report claims the American Heart Association entered into an agreement with J&J for their logo to be used on McNeil's Nicotrol for the price of $2.5 million annually.
They serve on each other's boards of directors. John Seffrin, CEO, ACS sits on the Board of Directors of Tobacco Free Kids [xxvi].
Public Library of Science Medicine (PLoS) this month published an article titled Global Health Philanthropy and Institutional Relationships: How should Conflicts of Interest Be Addressed [xxvii] which state "the Robert Wood Johnson Foundation has played a leading role in promoting anti-tobacco products and maintains Smoking Cessation Leadership Centres and programs, although its endowment is mainly invested in Johnson and Johnson, a leading manufacturer of cessation products, and some board members have been represented on both the Foundation's and the company's boards".
The British Medical Journal, April 14, 2011, published WHO (World Health Organization) Warns Anti-Smoking Campaigners Not to Become Too Close to Drug Firms [xxviii], ironically at a conference in Madrid sponsored by GSK, Pfizer and McNeil who market or own NRT.
Unfortunately, RWJF has used this footprint as a roadmap to further control our behaviours and bans of what they deem unhealthy. RWJF has given over half a billion dollars in obesity grants. First Lady Michelle Obama is the spokesperson for Childhood Obesity. RWJF fellow Shale Wong was assigned to the First Lady [xxix] (free of charge) 2009–2010. Experts argue for Tax on Sugar Sweetened Beverages, A RWJF publication [xxx]. Kelly Brownell, one of the experts of the two cited, claims taxing sugar-sweetened beverages would yield a 13% reduction whilst raising taxes. Ms. Brownwell is with Rudd Centre. The Rudd Centre for Food Policy and Obesity is a RWJF grant recipient of $5,842,740 [xxxi]. What really results from these types of bans and taxation is that industries and businesses fail and consumers are driven to alternative sweeteners, such as J&J's McNeil Company's SPLENDA.
This is the same playbook as their tobacco control playbook. I would look for RWJF to create and fund Sugar Free Kids. Who will be hurt are bakeries restaurants, bars (who can only sell "diet" pop with mixed drinks), and more. People will quit going to these businesses and will instead baker at home. Just like the smoking ban in Ohio cause 14.6 million more bottles of liquor to be sold for home and social gathering consumption.
Johnson and Johnson and RWJF get even richer from the sales of their products they've guaranteed through the laws they buy with their grants, fellows and partnerships. The more they make, the more money they have to buy more control of our lives. The word "lobbyist" may have a negative connotation, however they have to register and be known. "Fellows" assigned to influential Congressional Members and Committees are virtually unknown to the common American Citizen.
Foundations and Corporations do not get to make laws, especially when they profit from those laws, Ohio lawmakers work for us, not these profitable non-profits. WE have the power to vote lawmakers out, not foundations and NGOs. God gave us rights over ourselves and He gave us the power to make decisions for ourselves. That includes deciding whether to drink a sugary drink or patronise a smoking bar. The more these people try to rule our lives, the more resistance they'll get from larger and larger and larger groups of people.
Twenty-one people in nine states have filed complaints with Congressional Committees asking for an investigation into RWJF/J&J. J&J just settled for small fines rather than do prison time for bribery charges in a foreign country. I think what they've done to free market enterprise, artificial stock manipulation, insider trading, violation of the Sherman Act, violation of the RICO Act, legislative rent seeking and violation of the False Claims Act should no longer have the blind eye of Congress turned away. This article only barely touches on what we've discovered (including the 98.4% failure rate of NRT patches, the highly addictive properties of NRT gum). We look forward to the Ohio Supreme Court hearing the Zenos case. Ohio's Constitution is much more protective of property rights than the US Constitution. We can't wait to have our properties returned to their rightful owners! We want you, our state legislators, to know that you've supported these special interest groups over us mom and pop business owners. You've forgotten to protect the minority. You've forgotten that our properties are to be held forever inviolate. That's "forever", not ignored when it suits special interests. No one is forced to work for us and no one is forced to enter our properties. We want to be profitable once again. And we want you to know that we know who's behind controlling our behaviours for profit. Now ... do you want to side with them? Or us, the people who vote?
[i] http://en.wikipedia.org/wiki/Robert_Wood_Johnson_Foundation
[ii] http://www.fundinguniverse.com/company-histories/Robert-Wood-Johnson-Foundation-Company-History.html
[iii] http://www.rwjf.org/files/research/2009.rwjf.financial.statements.pdf
[iv] http://www.rwjf.org/files/publications/books/2005/chapter_01.pdf
[v] http://www.rwjf.org/programareas/grant.jsp?id=63261&pid=1141
[vi] http://www.rwjf.org/programareas/grant.jsp?id=63263&pid=1141
[vii] http://www.rwjf.org/grants/grant.jsp?id=41244
[viii] http://www.tobaccofreekids.org/press_releases/post/id_1077
[ix] http://publichealthlawcenter.org/programs/tobacco-control-legal-consortium
[x] http://smokingcessationleadership.ucsf.edu/BIoSteve.htm
[xi] http://www.attud.org/petition.php
[xii] http://www.srnt.org/about/supporters.cfm
[xiii] http://tobaccoscam.ucsf.edu/fake/index.cfm
[xiv] http://www.rwjf.org/programareas/resources/product.jsp?id=18079&pid=1141&gsa=1
[xv] http://www.legacyforhealth.org/593.aspx
[xvi] http://www.rwjf.org/grants/grant.jsp?id=61524
[xvii] http://www.rwjf.org/grants/grant.jsp?id=67571
[xviii] http://www.rwjf.org/files/publications/books/2005/chapter_01.pdf (pg 6)
[xix] http://en.wikipedia.org/wiki/Master_Settlement_Agreement
[xx] http://www.healthpolicyfellows.org/secure/alumni-search.php?action=search&keyword=&state=0&fellowship_year=2010&assignment=0&discipline=0
[xxi] http://www.nyc.gov/html/doh/downloads/pdf/smoke/smoke-nrt-faq.pdf
[xxii] http://www.cancer.org/acs/groups/content/@finance/documents/document/acsd-005945.pdf (pg 11)
[xxiii] http://www.cancer.org/acs/groups/content/@finance/documents/document/acsd-005945.pdf (pg 12)
[xxiv] http://www.cancer.org/acs/groups/content/@finance/documents/document/acsd-005945.pdf
(pg 20)
[xxv] http://opponentsofohiobans.com/Documents/ACS%20NRT%20table.doc
[xxvi] https://www.tobaccofreekids.org/content/who_we_are/annual_report/AnnualReport2010.pdf
[xxvii] http://www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.1001020
[xxviii] http://www.bmj.com/content/342/bmj.d2430.extract
[xxix] http://www.healthpolicyfellows.org/secure/alumni-bio.php?id=4591
[xxx] http://www.rwjf.org/childhoodobesity/digest.jsp?id=10245
[xxxi] http://www.rwjf.org/grants/grant.jsp?id=65013
Bar closures heavier in cities
A report out today by CR Consulting shows the bar closures throughout the UK, and concludes that contrary to expectation urban pubs have suffered more than rural and suburban ones. The populations affected are younger with larger concentrations of smokers. The report also shows how closures have accelerated since the smoking bans in Scotland, Wales, England and Northern Ireland. Data shown for all regions of the United Kingdom.
Comment from Forest and Scottish Licensed Trade Association here.
Comment from Forest and Scottish Licensed Trade Association here.
National Federation of Retail Newsagents complains at extent of ASH influence: Liberal Vision
Good for Liberal Vision for reporting this letter from the NFRN to the Prime Minister complaining about the close relationship between the Health Minister and Action on Smoking and Health:
This statement and public acceptance and deliverance of awards to an organisation that has been lobbying her department, MPs and other government departments (and indeed is granted government funding on the basis that it not be used for lobbying purposes) has called into question the manner in which recent tobacco display ban legislation has been made; and the ability of the Minister to be considered unbiased on the issue.
I attach a copy of the event report from an independent parliamentary reporting service and would ask that you formally conduct an investigation into the conduct of your minister in the light of her public admission that she had worked with an officer of an ASH funded parliamentary lobby group on recent legislation “behind the scenes”. Moreover, this inappropriate conduct necessitates a review of the legitimacy of the legislation itself. [emphasis added]
[...]
In light of these recent statements, I regrettably now see proof of these suspicions which is deeply offensive to our members who have campaigned so hard to see the government fulfil its pre-election commitments to bring the debate back to the House of Commons for a free vote and which the Conservatives and Liberal Democrats publically opposed in opposition.
[...]Writer Angela Harbutt also has hard words to say about ASH and its aims and working methods:
ASH receives huge amounts of money from the taxpayer and sadly, like so many publicly funded bodies with too much money and too little scrutiny it has NOT gone about its task well. ASH has now become a fat, over-staffed, political, and single-minded organisation hell bent on eradicating smoking from the face of the earth, by whatever means necessary. Where it could have worked with the industry to find solutions to the issues, it has set itself up against the manufacturers, the retailers and the consumers. And much of its so-called advice has been at best ineffective, and all too often counter-productive, with huge financial and social unintended consequences.ASH's destructive behaviour is of course in line with the Framework Convention on Tobacco Control. It does not sit well with ASH's original remit, as Angela Harbutt points out in the comments below:
As I understood it ASH was set up in 1971 as a campaigning health charity to work towards eliminating THE HARM caused by tobacco – not created to work towards eliminating tobacco. If that remains their public aim then working with the industry is surely a pretty sensible thing to do?Angela ... come to Scotland!
Wednesday, 22 June 2011
Ten-minute rule motion passed to ban smoking in cars: let's get some perspective
At Westminster today a Bill was approved that would ban smoking in cars carrying children. As a backbencher's Bill it collected less than 150 votes, but it got media attention because of its subject matter including mainstream attention from the BBC and ITV (among others) and the blogosphere, where it attracted the attention of Big Brother Watch.
The argument goes that having protected adults from secondary smoke, we must now protect children. But legislation banning smoking in enclosed public places has existed in the Republic of Ireland since 2004. At this time they were beginning to think of introducing it to Scotland and legislation to do this was passed in 2005, around six years ago. In other words it has taken the great and the good over six years to come to the conclusion that what might hurt adults in areas they need not go, might also hurt children in areas where they have no choice about going.
The real issue is of course that they could almost get off with designating private businesses as 'public places', but public opinion had not caught up with the idea that you can interfere with the smoking habits in the undeniably private areas of the home and car. Having established the right of interference in quasi-public places, their courage (if you can call it that) is growing. It has nothing to do with the level of risk involved, or the vulnerability of those affected, and everything to do with a steady process of invading autonomy in businesses, then in family cars, then in family homes.
How can you say in July 2005: 'the risk of exposure is unacceptable. We'll ban it with effect from next March'? There are other ways of handling bans of risky commodities, that leave you in little doubt that the government actually believes there is a risk and isn't just trying to mess you about.
The risk itself? The UK has a poor record on clean air quality, and it is to be expected that the government will concentrate its 'air quality' efforts on the smoking issue. This typifies the focus on lifestyle issues now being taken by global bodies, including the World Health Organisation, which has recently been trying to ratchet up interest in non-communicable diseases. This effort is reflected in the media by stories such as Unhealthy lifestyles to kill 52 million yearly by 2030. Such stories may not reflect the intention of the World Health Organisation (who knows?), but this one says that 'most' chronic diseases are caused by 'unhealthy and ethically wanting lifestyles'.
It looks as if they intend to blame the poor for getting ill needlessly. But they still want to treat those conditions that the poor would not be getting if only they behaved themselves. Is someone making money out of this?
The truth of course is that while lifestyle factors may contribute to ill health and many non-communicable diseases, there is no certainty about how much. It is not known to what environmental and other hazards workers, urban dwellers or other groups are exposed ('developing countries' include most of the world's population and a vast variety of working and living conditions), and while it might sound catchy to say that lifestyle factors are a common cause in their sicknesses, it is also profoundly lazy. Public policy will become limited to warnings about lifestyle issues, rather than awareness training about environmental issues and hazards at the workplace, for example. I hasten to add that I am guessing, but it looks like the World Health Organisation is taking a moralistic, judgemental and simplified approach to the issue of non-communicable diseases, rather than a scientific, measured one. And as we have already established, non-communicable diseases kill older people and people in wealthier parts of the world, more often than infants and young adult breadwinners. The 'paradigm shift' in the focus of pharmaceutical companies might be good for their balance sheets – will it result in improved conditions for people, or neglect for their most basic needs?
The argument goes that having protected adults from secondary smoke, we must now protect children. But legislation banning smoking in enclosed public places has existed in the Republic of Ireland since 2004. At this time they were beginning to think of introducing it to Scotland and legislation to do this was passed in 2005, around six years ago. In other words it has taken the great and the good over six years to come to the conclusion that what might hurt adults in areas they need not go, might also hurt children in areas where they have no choice about going.
The real issue is of course that they could almost get off with designating private businesses as 'public places', but public opinion had not caught up with the idea that you can interfere with the smoking habits in the undeniably private areas of the home and car. Having established the right of interference in quasi-public places, their courage (if you can call it that) is growing. It has nothing to do with the level of risk involved, or the vulnerability of those affected, and everything to do with a steady process of invading autonomy in businesses, then in family cars, then in family homes.
How can you say in July 2005: 'the risk of exposure is unacceptable. We'll ban it with effect from next March'? There are other ways of handling bans of risky commodities, that leave you in little doubt that the government actually believes there is a risk and isn't just trying to mess you about.
The risk itself? The UK has a poor record on clean air quality, and it is to be expected that the government will concentrate its 'air quality' efforts on the smoking issue. This typifies the focus on lifestyle issues now being taken by global bodies, including the World Health Organisation, which has recently been trying to ratchet up interest in non-communicable diseases. This effort is reflected in the media by stories such as Unhealthy lifestyles to kill 52 million yearly by 2030. Such stories may not reflect the intention of the World Health Organisation (who knows?), but this one says that 'most' chronic diseases are caused by 'unhealthy and ethically wanting lifestyles'.
It looks as if they intend to blame the poor for getting ill needlessly. But they still want to treat those conditions that the poor would not be getting if only they behaved themselves. Is someone making money out of this?
The framework confirms the industry’s crucial role in continued investment in R&D programmes to develop drugs for the prevention and treatment of non-communicable disease, with over 1,500 products in the pipeline currently. It also commits the industry to target its innovation towards the specific needs of the developing world. To this end, in addition to the framework, there will be a programme of research, to improve understanding of the specific needs of developing world populations. [emphasis added]Yes, there might be some very lucrative contracts here ... prevention and treatment of conditions that are killing off people in vast quantities (conditions that the patients bring on themselves, let's not forget!). The paragraph quoted above reads almost like a business plan for pharmaceutical companies.
The truth of course is that while lifestyle factors may contribute to ill health and many non-communicable diseases, there is no certainty about how much. It is not known to what environmental and other hazards workers, urban dwellers or other groups are exposed ('developing countries' include most of the world's population and a vast variety of working and living conditions), and while it might sound catchy to say that lifestyle factors are a common cause in their sicknesses, it is also profoundly lazy. Public policy will become limited to warnings about lifestyle issues, rather than awareness training about environmental issues and hazards at the workplace, for example. I hasten to add that I am guessing, but it looks like the World Health Organisation is taking a moralistic, judgemental and simplified approach to the issue of non-communicable diseases, rather than a scientific, measured one. And as we have already established, non-communicable diseases kill older people and people in wealthier parts of the world, more often than infants and young adult breadwinners. The 'paradigm shift' in the focus of pharmaceutical companies might be good for their balance sheets – will it result in improved conditions for people, or neglect for their most basic needs?
Tuesday, 21 June 2011
Ohio smoking ban: unpaid fines and cuts in enforcement
The state of Ohio is seeing cutbacks in smoking ban enforcement. Enforcement is also sketchy – thousands of dollars are outstanding in unpaid fines.
Landlords rather than individual smokers have been leant on by the law:
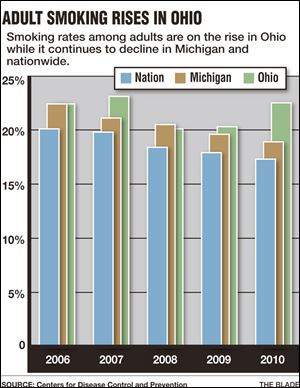
On top of the other problems faced by the health department in Ohio, smoking rates are not even declining – in fact they are going up, and local smoking cessation services have also taken a hit in the budget cuts.
Landlords rather than individual smokers have been leant on by the law:
Many neighborhood bars and other smoking-ban opponents continue to hold out against the law, which was built around using fines to help pay for enforcement. Among their assertions is that the ban is unconstitutional, as enforcement has focused on fining business owners, not actual smokers as allowed by the law. [...]
If bar owners put signs up about the smoking ban, remove ashtrays, and take other measures to notify patrons that smoking isn't allowed in their establishments, they should not be fined, Mr. Thompson said. Smokers breaking the ban should be fined by health departments, but are not, he said.
"They're just picking and choosing what part of the law they want to enforce," Mr. Thompson said.Picking on landlords is a trait I seem to call here in the UK too. During a visit of enforcement officers, 'Customers were spotted smoking in full view of staff, who made no attempt to stop them, the court heard.' Not content with making it a crime to smoke in an enclosed public place (sic), the law made it a crime to allow smoking in such a public place. Easy pickings maybe, but unfairly selective, and it is small wonder that it is dubbed unconstitutional. In the UK it's the way to get the ban enforced, but it seems that Ohio residents are more obstructive when they feel abused by the authorities.
On top of the other problems faced by the health department in Ohio, smoking rates are not even declining – in fact they are going up, and local smoking cessation services have also taken a hit in the budget cuts.
{kind=link}
Monday, 20 June 2011
Lord suspends judgement in dismissing tobacco vending machine appeal
Suspends judgement? well that's remarkably what it looks like. Lord Neuberger's words have been widely quoted:
It seems that all you have to do is come up with an idea to improve public health, and bring children into the discussion, and the courts won't even bother listening to any of your adversaries. Self-evidently. But when jobs are at stake, surely guesswork isn't enough.
I thought the whole point of having three arms of government (the separation of powers) was to protect the integrity of government by ensuring that each arm did its job properly.
Imperial Tobacco intends to appeal to the Supreme Court.
virtually any measure which a government takes to restrict the availability of tobacco products, especially to young people, is almost self-evidently one with which no court should interfere.Although stating that DoH statistics were 'little more than guesses', His Lordship reckons that the government has no case to answer simply by virtue of being government promoting health. Regardless of the number of jobs at stake, there is no point in anyone even trying to bring a case against the government because ... yes ...
virtually any measure which a government takes to restrict the availability of tobacco products, especially to young people, is almost self-evidently one with which no court should interfere.Some of the public commenting in both the Daily Mail and the Sun (and no doubt elsewhere) struggle to understand why age-restriction technology (for instance radio-controlled vending machines) may not be used. It may not be 100 per cent fool proof (although it probably comes quite close) but neither is banning vending machines. The children and young adults of the future won't even miss them – they are too expensive even for adults to use as a regular source of supply.
It seems that all you have to do is come up with an idea to improve public health, and bring children into the discussion, and the courts won't even bother listening to any of your adversaries. Self-evidently. But when jobs are at stake, surely guesswork isn't enough.
I thought the whole point of having three arms of government (the separation of powers) was to protect the integrity of government by ensuring that each arm did its job properly.
Imperial Tobacco intends to appeal to the Supreme Court.
Spanish campaigners and others seek to follow example of Netherlands tobacco policy
Translated by Google, read this Spanish blog post. Beginning with the withdrawal of Dutch public funding from mass smoking cessation campaigns, the piece goes on to discuss the smoking ban itself.
As Scotland's licensed trade has requested, as a campaign orchestrated by Forest at Westminster will put forward at a meeting on 29 June (follow the link for information and to register for attendance).
Edith Schippers is the Minister of Health, which reversed the ban on smoking in the Dutch hotel, with reasoning also flawless. If you smoke in hospitality venues in defense of labor rights of workers, provided that the establishment does not have employees, must be owner's decision whether to smoke or not smoke inside. We want the same for Spain.Pointing out that the WD party in the Netherlands gained electoral support on the smoking ban issue, the article points out that what the Netherlands can do, Spain can also do. As Nevada has done in its own way.
As Scotland's licensed trade has requested, as a campaign orchestrated by Forest at Westminster will put forward at a meeting on 29 June (follow the link for information and to register for attendance).
Nevada allows food service in (smoking) bars
Acting on representations from the catering and hospitality trade Nevada prepares to allow food service in bars, and smoking in family restaurants where a separate room is available.
It appears that in Nevada, it is accepted that smoking restrictions (forcing establishments to choose between allowing smoking and providing a food service) have led to sharp drops in income for businesses. No guff about supermarket prices here.
The overturned bill that voters approved in 2006 banned the provision of food by smoking taverns. Although unlike Scottish law it allowed some provision for smokers, it still cost the hospitality industry heavily. More here. Here. the American Lung Association is protesting about potential loss of life – a tad melodramatically, since secondary smoke is certainly not as lethal as they claim and quite possibly not lethal at all. Furthermore, nobody is banning the provision of proper air management/cleaning systems that clean air thoroughly.
More again here, from Marcus Aurelius, including a link on undue influence (Nicorette).
It appears that in Nevada, it is accepted that smoking restrictions (forcing establishments to choose between allowing smoking and providing a food service) have led to sharp drops in income for businesses. No guff about supermarket prices here.
The overturned bill that voters approved in 2006 banned the provision of food by smoking taverns. Although unlike Scottish law it allowed some provision for smokers, it still cost the hospitality industry heavily. More here. Here. the American Lung Association is protesting about potential loss of life – a tad melodramatically, since secondary smoke is certainly not as lethal as they claim and quite possibly not lethal at all. Furthermore, nobody is banning the provision of proper air management/cleaning systems that clean air thoroughly.
More again here, from Marcus Aurelius, including a link on undue influence (Nicorette).
Sunday, 19 June 2011
Public health minister Anne Milton presents at Smoking Cessation Conference
Public Health Minister Anne Milton recently presented Action on Smoking on Health with an award from the World Health Organisation at a recent meeting of the All-party Parliamentary Group on Smoking and Health.
This last week she is listed as presenting at the UK National Smoking Cessation Conference, in a piece entitled The future for tobacco control and smoking cessation in England: Our vision for the next 5 years. It's one of the few presentation that doesn't get its own summary page on the website, so we'll have to wait until all the presentations are made available in several weeks before finding out what she said.
So much for advice from the top to anti-smoking activists not to cosy up to drugs companies.
This last week she is listed as presenting at the UK National Smoking Cessation Conference, in a piece entitled The future for tobacco control and smoking cessation in England: Our vision for the next 5 years. It's one of the few presentation that doesn't get its own summary page on the website, so we'll have to wait until all the presentations are made available in several weeks before finding out what she said.
So much for advice from the top to anti-smoking activists not to cosy up to drugs companies.
Saturday, 18 June 2011
Europe launches 'Ex-smokers are unstoppable', 3 year campaign
(and in case you think that is grotesque, try this)
The three-year anti-smoking campaign involves an interactive programme called iCoach, an application designed to encourage smokers to keep on trying to stop smoking. EU officers will be encouraged to lead by example and register with iCoach before it is let loose on the public. It has been published in all the European languages (you can see why the campaign is expected to cost 16 million euros).
As well as putting pressure on officers to sign up to this hideously expensive campaign in order to set an example to lesser mortals who don't work for it, EU Health Commissioner John Dalli also looks forward to extending legislation restricting the use of smokeless tobacco products. So not only will they resort to bullying EU employees, they will also seek to ban e-cigarettes and similar products and push for further restrictions on the marketing and selling of tobacco.
The more I read the less I understand how the smoking cessation racket has been sold on the public. Courtesy of Rick S's comment yesterday, have a look at this on the views of Robert West from 2007. Robert West is a professional anti-tobacco activist, as the article makes clear. Interviewed at the very start of the English smoking ban, he says this:
The three-year anti-smoking campaign involves an interactive programme called iCoach, an application designed to encourage smokers to keep on trying to stop smoking. EU officers will be encouraged to lead by example and register with iCoach before it is let loose on the public. It has been published in all the European languages (you can see why the campaign is expected to cost 16 million euros).
As well as putting pressure on officers to sign up to this hideously expensive campaign in order to set an example to lesser mortals who don't work for it, EU Health Commissioner John Dalli also looks forward to extending legislation restricting the use of smokeless tobacco products. So not only will they resort to bullying EU employees, they will also seek to ban e-cigarettes and similar products and push for further restrictions on the marketing and selling of tobacco.
The more I read the less I understand how the smoking cessation racket has been sold on the public. Courtesy of Rick S's comment yesterday, have a look at this on the views of Robert West from 2007. Robert West is a professional anti-tobacco activist, as the article makes clear. Interviewed at the very start of the English smoking ban, he says this:
The experience of the smoking ban in Ireland and elsewhere suggests that the ban itself will have limited impact on the government target of 21 per cent smoking prevalence by 2010. Around 25 per cent of people in England admit to smoking cigarettes. To cut this figure by one per cent, every single smoker in the country would have to try to stop, and at least half of them would have to use effective treatments to help them do it.
“The government is looking for a miracle, basically. But the point is not whether we will reach arbitrary targets but the fact that for every one per cent of smokers we see about 3,000 unnecessary deaths per year. Everything we can do to bring down the figure means a lot of suffering prevented.”Even a professional anti-smoker believes that the success rate in smoking cessation is very low. People like West truly believe that only by all smokers attempting to stop smoking at the same time can a drop of 1 per cent in the smoking rate be achieved, and that this will somehow save 3,000 lives a year. The last sentence seems to be mere window dressing. If that's what it takes to bring smoking rates down, they clearly can't be coming down very much, and all the efforts going into smoking cessation programmes are doing little besides boosting pharmaceutical takings, and propping up the careers of professional anti-smoking activists like Robert West.
Friday, 17 June 2011
A note on spam and unpublished comments – to Anonymous
I have today chanced on a list of posts in the admin area of this blog that Blogspot designated as spam and didn't publish. There were 33 items in the list. Many were from a contributor or contributors called Anonymous, and clearly s/he/they had tried to publish two or three more than once.
I have now published all of them that were not actual spam. I am only sorry I didn't pick up on it earlier and I hope that Anonymous will forgive me and post again!
I have now published all of them that were not actual spam. I am only sorry I didn't pick up on it earlier and I hope that Anonymous will forgive me and post again!
Thursday, 16 June 2011
Yet another problem with Champix (cardiovascular)
Reports today indicate slightly raised risks of cardiovascular problems. A recent trial of patients with cardiovascular disease showed patients taking Champix were slightly more likely to experience heart problems than those taking a placebo.
Written warnings accompanying the drug will warn patients of this risk and Pfizer will be required by the FDA to carry out further studies in order to establish the risk more clearly.
The risk is said to be 'small' – that will surprise no one! What beats me is why anyone will take it for such a limited outcome:
Written warnings accompanying the drug will warn patients of this risk and Pfizer will be required by the FDA to carry out further studies in order to establish the risk more clearly.
The risk is said to be 'small' – that will surprise no one! What beats me is why anyone will take it for such a limited outcome:
An independent randomized trial of 700 smokers with cardiovascular disease who were treated with Chantix or a placebo showed that Chantix was effective in helping patients quit smoking for as long as one year. [emphasis added]Other problems are by now well documented:
Chantix has been associated with agitation, depression and suicidal thoughts, and, in clinical trials, linked with nightmares. Psychiatric symptoms have occurred in people without a history of mental illness and have worsened in people who already had mental illness. [emphasis added]To this, we can add an apparent cover up of adverse incidents involving Champix.
Federal Food and Drug Administration officials acknowledged that they asked Pfizer to resubmit thousands of records after realizing that the company was sending required reports in an inappropriate format that could not be added to the agency’s Adverse Events Reporting System, or AERS.The French Health Minister has recently delisted Champix as a publicly funded drug. I put the point to the local NHS trust in Scotland, putting the point that the French Minister had banned the drug and requesting its withdrawal by NHS Lothian. Their reply follows:
The Scottish Government does not advise upon the licensing and safety of medicines since this is not a devolved power for the Scottish Government. As such, they are would not be in a position to withdraw this medicine from use across Scotland . The Medicines and Healthcare products Regulatory Agency (MHRA) is the UK organisation responsible for the licensing of medicines and monitoring of the safety of these medicines. Information on this organisation and its activities to ensure public safety with medicines can be found at http://www.mhra.gov.uk/index.htm
The MHRA has had varenicline under intensive surveillance for the last couple of years to ensure that the benefit to patients continues to outweigh any potential risks. They work in collaboration with the international drug safety monitoring network to ensure safety of medicines. A copy of an article writtten for their publication the Drug Safety Update on this can be seen at http://www.mhra.gov.uk/Safetyinformatio ... /CON087722 . They encourage all healthcare professionals and patients to be vigilant in reporting any suspected side effects with this medicine. Patients and healthcare professionals can report any suspected reactions for medicines at http://yellowcard.mhra.gov.uk/
At present there has not been any indication given by the MHRA that varenicline should not be used; but continued monitoring of safety is ongoing. Therefore it remains licensed for use within the UK . Prescribers have been made aware of the risk; and should be taking this into consideration when deciding if the potential benefit to the patient before prescribing for a patient. There is no move currently to discontinue use of the medicine in appropriate patients that are likely to recive benefit. If, however, there is additional warnings issued from the MHRA of safety concerns (or indeed recommend withdrawal from use), then NHS Lothian and all other Health Boards across Scotland would then comply.
I hope this information is of use to you.
Yours sincerely
Melinda Cuthbert
Lead Pharmacist Lothian Medicines Information Service/Yellow Card Centre Scotland, Pharmacy Department, Royal Infirmary of Edinburgh, Edinburgh EH16 4SAClearly MHRA needs to be notified of public concern. It is extraordinary that a drug with such effects is recommended, subsidised, to the general public, especially people with a psychiatric history, when even those without such a history are disturbed by it. ASH Scotland's most recent update (scroll down this link) on Champix and mental health says:
Clinical trials during drug development excluded patients with active psychiatric illnesses leaving the risks associated with varenicline use in this patient population unknown. A review of the evidence in Expert Opinion on Drug Safety has concluded that although the risk of potential neuropsychiatric events is evident through voluntary reporting systems and reported cases in the literature, multiple studies and case reports support the use of varenicline in the mental health population.As often, I take a diametrically opposing view.
Should tobacco control lead the fight against non-communicable diseases?
Unlike the Framework Convention for Tobacco Control I can't see the need for the fight against non-communicable diseases to be led by tobacco control. Tobacco control is a single issue – non-communicable diseases are various in their causes and manifestations.
Worldmapper sets out the incidence of non-communicable diseases across the world in some detail. Starting on this page we can see from a list how, with a broad brush, smoking-related deaths account for some four-fifths of non-communicable diseases. But start clicking on the maps (go to 'next map') featuring each kind of cancer, many cancers do not mention smoking as a factor, and the description of lung cancer mentions other significant risk factors. (Go here for a comprehensive index of causes of death.) In fact the FCA tells us that tobacco causes 1 in 6 deaths from non-communicable diseases (and that it makes people with other conditions more likely to die).
Aside from factors in deaths, when considering who should lead the global fight against non-communicable diseases, we should also consider the ages at which people die and tackle first those conditions that kill younger people rather than older ones. A very broad brush suggests that non-communicable diseases are less prevalent in countries where people tend to die at a younger age. From here, go to 'next map', keep clicking and you will see that the people who live longest die in the rich world ... obvious, but we are told that most deaths are from non-communicable diseases.
The Framework Convention Alliance's report is clearly geared to a market of concern for developing countries. I am already finding it difficult to see why tobacco control should lead 'the fight against non-communicable diseases'. Why should non-communicable diseases be prioritised if we are trying to save young breadwinners', children's and infants' lives in the poorest areas of the world? Surely there are diseases that afflict people in poor countries but they are not all tobacco related, and surely diseases that people can transmit to each other are far more dangerous anyway.
How about this for a reason to focus on tobacco control:
Worldmapper sets out the incidence of non-communicable diseases across the world in some detail. Starting on this page we can see from a list how, with a broad brush, smoking-related deaths account for some four-fifths of non-communicable diseases. But start clicking on the maps (go to 'next map') featuring each kind of cancer, many cancers do not mention smoking as a factor, and the description of lung cancer mentions other significant risk factors. (Go here for a comprehensive index of causes of death.) In fact the FCA tells us that tobacco causes 1 in 6 deaths from non-communicable diseases (and that it makes people with other conditions more likely to die).
Aside from factors in deaths, when considering who should lead the global fight against non-communicable diseases, we should also consider the ages at which people die and tackle first those conditions that kill younger people rather than older ones. A very broad brush suggests that non-communicable diseases are less prevalent in countries where people tend to die at a younger age. From here, go to 'next map', keep clicking and you will see that the people who live longest die in the rich world ... obvious, but we are told that most deaths are from non-communicable diseases.
The Framework Convention Alliance's report is clearly geared to a market of concern for developing countries. I am already finding it difficult to see why tobacco control should lead 'the fight against non-communicable diseases'. Why should non-communicable diseases be prioritised if we are trying to save young breadwinners', children's and infants' lives in the poorest areas of the world? Surely there are diseases that afflict people in poor countries but they are not all tobacco related, and surely diseases that people can transmit to each other are far more dangerous anyway.
How about this for a reason to focus on tobacco control:
Unlike malaria, AIDS or neglected tropical diseases, where the vector is a mosquito, virus or parasite, tobacco has a human vector in the shape of a wealthy, powerful, multinational industry. Tobacco industry revenue dwarfs the GDP of many countries and the industry has used its billions to aggressively market its products in low and middle income countries. As the world strives to reduce poverty, tackle the financial crisis, food insecurity and climate change, no country can afford the health, economic or environmental consequences of tobacco use. [...]We'll fight tobacco because it's represented by a human agent. They're bad people who profit from death ... unlike the poor mosquito? Forcing people to spend money on them ...
A unique feature of the tobacco pandemic is that after more than half a century of research and analysis, we know how to reduce this burden. Not only that, but we have an internationally negotiated, legally binding package of evidence-based tobacco control measures, the WHO Framework Convention on Tobacco Control, to which more than 170 WHO Member States are Parties, accounting for more than 85% of the global population.[but they don't know how to reduce the burden. All they do is to move it about – in fact they have shifted the burden of tobacco from the rich world to the poor world. They have banned advertising in one part of the world and splutter with indignation whenever tobacco companies find somewhere they are still allowed to advertise. In fact they still describe tobacco-related disease as 'preventable'.]
Effective tobacco control policies reduce NCDs: the incidence of cardiovascular and respiratory disease falls first, followed by cancer and other diseases.As exemplified by Jill Pell who discovered a 17 per cent reduction in heart attack admissions and an 18 per cent reduction in admissions for childhood asthma following the implementation of the smoking ban in Scotland,
... Health-care costs are reduced and productivity is increased. They can also generate significant government revenues. Increasing tobacco taxes does more than any other single measure, at least in the short term, to decrease tobacco use. Appropriately structured, tobacco taxes have the potential to pay for tobacco control, for action on other NCDs or for any other useful public purposes governments may choose.The triumph of hope over experience? Is there not something of a conflict of interest in relying on tobacco sales for funding to promote tobacco control? Spain has seen a price war in tobacco following its smoking ban ... isn't this a likely consequence of further increasing tobacco taxes?
Global tobacco control can and should be the lead engine
That is the conclusion of one of the world’s pre-eminent public policy institutions, the Center for Strategic and International Studies, in its analysis of the potential of the UN High-level Meeting on NCDs (19-20 September 2011) to elevate NCDs onto the global stage. Many of the world’s most knowledgeable scientists, key non-governmental organisations, and public health workers in low, middle and high income countries are already engaged in marshalling the data and proposing priority actions to make immediate and sustainable progress.The FCA document seems to do little but recommend a power grab by tobacco control interests, describing the Framework Convention on Tobacco Control to the exclusion of everything else, boasting of the success of tobacco control measures (in a box headed 'Evidence' but containing only assertions) – even offering a wild guess as to how many more people would survive tuberculosis if they didn't smoke. Remember Richard Horton's view:
Although 80% of NCD deaths take place in low and middle-income countries, the fact is that for the 50 or so poorest countries in the world an unfinished litany of problems remains—infectious diseases, maternal and childhood illnesses, and unchecked population growth. NCDs come bottom of this list.
The document insists that the measures described are cheap – but just because they are cheap does not mean they should be prioritised. Unfortunately the Framework Convention on Tobacco Control gives the FCA grounds to claim that countries have international obligations and have no choice on this issue. This should be viewed as a violation of national integrity by countries everywhere. In fact the creation of this treaty as the first binding multilateral treaty of the WHO should be cause for alarm. This document shows an over-riding concern to fight an industry rather than to tackle the complex issues surrounding premature death in the developing world.
Tuesday, 14 June 2011
ASH Scotland displays anti-smoking alliance building skills to London conference
Today was the second day of the 2011 UK Scottish Smoking Cessation Conference. Scottish readers will be proud to learn that the day kicked off with a workshop on successful tobacco control alliances, led by David Robertson, Alliances Manager and STCA Coordinator, ASH Scotland.
Building such alliances form a large part of ASH Scotland's work. The latest Local Tobacco Alliances project report describes work done over the last five years (this round of funding finishes this year). The alliances appear to include different professional and voluntary groups (predominantly in social services, health, environmental services). The report is full of the usual self-congratulatory waffle, but a more detailed idea of what the alliances do can be found here – a huge array of smoking cessation advice delivered to people of all ages and every conceivable setting.
I wish I could feel proud of such teamwork But – as the project documentation shows – this is top-down government starting with the World Health Organisation. It's about employing civil society to pursue a global goal, almost independently of the Scottish Government (that is, they pay a substantial whack of ASH Scotland's income) – and where's the accountability in that?
Building such alliances form a large part of ASH Scotland's work. The latest Local Tobacco Alliances project report describes work done over the last five years (this round of funding finishes this year). The alliances appear to include different professional and voluntary groups (predominantly in social services, health, environmental services). The report is full of the usual self-congratulatory waffle, but a more detailed idea of what the alliances do can be found here – a huge array of smoking cessation advice delivered to people of all ages and every conceivable setting.
I wish I could feel proud of such teamwork But – as the project documentation shows – this is top-down government starting with the World Health Organisation. It's about employing civil society to pursue a global goal, almost independently of the Scottish Government (that is, they pay a substantial whack of ASH Scotland's income) – and where's the accountability in that?
Monday, 13 June 2011
Dutch cut back on smoking cessation
I have learned over the last few years to become very cautious on the issue of universal health benefits – getting all medication free at point of need. Being congenitally hypothyroid I got everything I needed (for that condition) free even before the Scottish Government made everything free. The point is that I believe everyone should have the right to life-saving drugs – the problem is that when the state provides health care, it also decides what is essential, what you need. That is why it can criminalise somebody for treating themselves with cannabis for multiple sclerosis yet think nothing of prescribing Champix, or ritalin for kids, or countless other pharmaceutical remedies that someone else has decided society 'needs' so much that it should get it without the individual paying for it. The beneficiaries of this arrangement are easily identified and less easily satisfied with their stupendous market share in medicines.
In the Dutch case, they are definitely doing what they should be doing in Scotland, and axing subsidised smoking cessation. Anyone who wants to give up smoking needs a lot of will power.Many people can do it without drugs if they want to do it at all. This is not denying anyone treatment for leprosy, malaria, AIDS, tuberculosis, or any other life-threatening condition. It's withdrawal of health budget money from behavioural change, which is acknowledged by practitioners not to be effective.
The United Kingdom National Smoking Cessation Conference started today, with 603 delegates learning all the tricks of the trade. For example, they plan to teach 'disadvantaged carers' (single parents?) how to exercise TA (temporary abstinence) using NRT (nicotine replacement therapy) so as not to hurt their kids – anti-smokers' peculiar idea of harm reduction (take a pharmaceutically prepared substitute). I have my own feelings about these campaigns to stop people smoking at home. But that aside, the money spent on smoking cessation would be better spent on almost any other aid, not only for disadvantaged carers of children but also of carers of people with dementia, many of whom who are likely to be elderly themselves instead of all these resources invested in stopping people from smoking.
I don't know how far the Dutch cuts go, but insofar as they stop supporting this appalling market in NRT and related medications, I'm with them.
In the Dutch case, they are definitely doing what they should be doing in Scotland, and axing subsidised smoking cessation. Anyone who wants to give up smoking needs a lot of will power.Many people can do it without drugs if they want to do it at all. This is not denying anyone treatment for leprosy, malaria, AIDS, tuberculosis, or any other life-threatening condition. It's withdrawal of health budget money from behavioural change, which is acknowledged by practitioners not to be effective.
The United Kingdom National Smoking Cessation Conference started today, with 603 delegates learning all the tricks of the trade. For example, they plan to teach 'disadvantaged carers' (single parents?) how to exercise TA (temporary abstinence) using NRT (nicotine replacement therapy) so as not to hurt their kids – anti-smokers' peculiar idea of harm reduction (take a pharmaceutically prepared substitute). I have my own feelings about these campaigns to stop people smoking at home. But that aside, the money spent on smoking cessation would be better spent on almost any other aid, not only for disadvantaged carers of children but also of carers of people with dementia, many of whom who are likely to be elderly themselves instead of all these resources invested in stopping people from smoking.
I don't know how far the Dutch cuts go, but insofar as they stop supporting this appalling market in NRT and related medications, I'm with them.
Sunday, 12 June 2011
Too little too late: Duffy answers Waterson
The response, when it came, was barely audible. Sheila Duffy's retaliation to Paul Waterson's suggestion that perhaps we should review the smoking ban came five days later, and somewhat tepidly reiterating the same tired points that we have been hearing for years now.
The smoking ban reduced heart attack admissions by 17 per cent in the year following implementation. Except they didn't, as was blindingly obvious from the moment Jill Pell's study was announced to the world (nine months before the actual study was published).
Asthma attacks in children declined by 18 per cent (the smoking ban did not affect child venues) – this was not true either.
Duffy also remarks on the state of the hospitality sector, remarking that it has not suffered overall. However, certain sections have suffered, namely pubs, clubs and bingo halls. The licensed trade association would not be calling for a review if its members were not suffering.
Duffy finally asks 'who would compromise or roll back on these health gains'? The problem has been that she and her like have lost much credibility over these supposed health gains. Consider ASH Scotland's next project: extending the smoking ban to prisons and mental institutions and intervening to stop people from smoking with children at home. It's the issue of children that exposes the poverty of the secondary smoking claims. It is an article of faith among anti-smoking activists that smoking bans do not increase children's exposure to secondary smoke. But the smoking ban inevitably involved at least the risk to children of considerably more exposure to secondary smoke. Since the strategy was denormalising smoking, the politically acceptable route was to prohibit smoking in public places and then conduct a very thorough 're-education' to persuade parents not to smoke at home. (Coming soon to a town near you.) It might have been more credible simply to have made some very strong statements about secondary smoke to encourage parents to smoke away from home, but left adult venues alone, with perhaps some encouragement to use extraction systems. That would have both reinforced smoking as an adult activity and protected children further from exposure to smoke – but of course would not have 'denormalised' smoking or made smokers an object of public vilification.
As a rebuttal of Paul Waterson's piece, Sheila Duffy's fails: Mr Waterson's is better researched and more reasonable. I would not agree with his recommendation of separate smoking rooms, unless he wants bars hit with rules from licensing boards about when staff may enter specific rooms in pub premises. An indoor air quality standard and extraction systems could do the job, clear the air of all the stale air as well as the smoke, and open up pubs for business to their core punters again.
The smoking ban reduced heart attack admissions by 17 per cent in the year following implementation. Except they didn't, as was blindingly obvious from the moment Jill Pell's study was announced to the world (nine months before the actual study was published).
Asthma attacks in children declined by 18 per cent (the smoking ban did not affect child venues) – this was not true either.
Duffy also remarks on the state of the hospitality sector, remarking that it has not suffered overall. However, certain sections have suffered, namely pubs, clubs and bingo halls. The licensed trade association would not be calling for a review if its members were not suffering.
Duffy finally asks 'who would compromise or roll back on these health gains'? The problem has been that she and her like have lost much credibility over these supposed health gains. Consider ASH Scotland's next project: extending the smoking ban to prisons and mental institutions and intervening to stop people from smoking with children at home. It's the issue of children that exposes the poverty of the secondary smoking claims. It is an article of faith among anti-smoking activists that smoking bans do not increase children's exposure to secondary smoke. But the smoking ban inevitably involved at least the risk to children of considerably more exposure to secondary smoke. Since the strategy was denormalising smoking, the politically acceptable route was to prohibit smoking in public places and then conduct a very thorough 're-education' to persuade parents not to smoke at home. (Coming soon to a town near you.) It might have been more credible simply to have made some very strong statements about secondary smoke to encourage parents to smoke away from home, but left adult venues alone, with perhaps some encouragement to use extraction systems. That would have both reinforced smoking as an adult activity and protected children further from exposure to smoke – but of course would not have 'denormalised' smoking or made smokers an object of public vilification.
As a rebuttal of Paul Waterson's piece, Sheila Duffy's fails: Mr Waterson's is better researched and more reasonable. I would not agree with his recommendation of separate smoking rooms, unless he wants bars hit with rules from licensing boards about when staff may enter specific rooms in pub premises. An indoor air quality standard and extraction systems could do the job, clear the air of all the stale air as well as the smoke, and open up pubs for business to their core punters again.
Thursday, 9 June 2011
Plain packaging and intellectual property arguments
Professor Simon Chapman, a tobacco control careerist, defends plain packaging with vigour. He believes that the worries of intellectual property experts, the British, French, Canadian and Lithanian governments and an Australian senate report dating back to 1995 are misplaced, on both the advisability of the policy and its potential to create positive health outcomes. Just yesterday we reported how concern about this policy has reached Washington.
I'm no policy expert but its seems to me that no government should expect to wipe out the brand identity of products and not expect manufacturers to react with court action. It amounts to destruction of property, on a vast scale. As discussed in the clip below, possessing intellectual property (and this includes branding) implies being able to trade on it. Simon Chapman's argument appears to be that if the government destroys brands without either itself or a third party gaining directly from their destruction this is somehow allowable. It's okay as long as the government doesn't take these brands for its own use, or give it away to another party. Quoting Professor Mark Davison, Chapman explains:
The discussion is well worth a listen – Professor Bennett points out that plain packaging will create two classes of intellectual property holders, namely tobacco companies, who are not allowed to exploit their intellectual property, and all other intellectual property holders, who can exploit their brands and trade marks to make as much money as they wish. Since even Australian Health Minister Nicola Roxon knows there is no empirical evidence that plain packaging will work, since it has never been tried before, it is hard to say that there will be any public health benefit. Arbitrarily destroying a single industry's property when nobody benefits does seem to be pointless at best, and vindictive at worst. I think I prefer Alan Bennett's reasoning to Simon Chapman's. I hope he's right anyway.
LATE EDIT – a group of tobacco-producing nations led by the Dominican Republic has also spoken against the policy at a meeting of the World Trade Organisation in Geneva – concerned about damage to the tobacco trade. Confusing intention with effect, the Australian trade minister described the move as 'not anti-trade' but 'anti-cancer'. The idea of the policy is to prevent tobacco purchasers paying more because they like specific brands – it will bring tobacco prices down. Its effect is more likely to be anti-trade and (if tobacco is as dangerous as they say it is) pro-cancer!
I'm no policy expert but its seems to me that no government should expect to wipe out the brand identity of products and not expect manufacturers to react with court action. It amounts to destruction of property, on a vast scale. As discussed in the clip below, possessing intellectual property (and this includes branding) implies being able to trade on it. Simon Chapman's argument appears to be that if the government destroys brands without either itself or a third party gaining directly from their destruction this is somehow allowable. It's okay as long as the government doesn't take these brands for its own use, or give it away to another party. Quoting Professor Mark Davison, Chapman explains:
"The extinction of rights or the reduction of rights is not relevant. The government or a third party must acquire property as a consequence of the legislation.
“The government does not wish to use the tobacco trade marks. Nor does it want third parties to do so. It does not desire to or intend to acquire any property. The proposition that prohibitions on the use of property do not constitute an acquisition of property was confirmed by the High Court as recently as 2009. In that case, the High Court held that the government was entitled to extinguish property rights in licences of farmers to take bore water.”The implication that government can actually destroy property (intellectual or otherwise) if it can satisfy a court that it doesn't accrue any direct benefit does not reassure many of the opponents of plain packaging, many of whom fear that legal action could result in enormous pay-outs that the taxpayer will ultimately have to pay. This is the line of radio presenter Alan Jones (a self-confessed smoke-hater, but he explores this issue with an open mind – on smoke, anyway!) in this discussion with Alan Bennett, adjunct professor of law at Sydney University. (Much of the same material is covered here.) Jones discusses many angles, including the lack of evidence that plain packaging will reduce smoking rates, and international concern about trade related property rights agreements (TRIPS is a World Trade Organisation ruling).
The discussion is well worth a listen – Professor Bennett points out that plain packaging will create two classes of intellectual property holders, namely tobacco companies, who are not allowed to exploit their intellectual property, and all other intellectual property holders, who can exploit their brands and trade marks to make as much money as they wish. Since even Australian Health Minister Nicola Roxon knows there is no empirical evidence that plain packaging will work, since it has never been tried before, it is hard to say that there will be any public health benefit. Arbitrarily destroying a single industry's property when nobody benefits does seem to be pointless at best, and vindictive at worst. I think I prefer Alan Bennett's reasoning to Simon Chapman's. I hope he's right anyway.
LATE EDIT – a group of tobacco-producing nations led by the Dominican Republic has also spoken against the policy at a meeting of the World Trade Organisation in Geneva – concerned about damage to the tobacco trade. Confusing intention with effect, the Australian trade minister described the move as 'not anti-trade' but 'anti-cancer'. The idea of the policy is to prevent tobacco purchasers paying more because they like specific brands – it will bring tobacco prices down. Its effect is more likely to be anti-trade and (if tobacco is as dangerous as they say it is) pro-cancer!
Wednesday, 8 June 2011
Imperial Tobacco attacks Welsh tobacco control policy
This has been reported on at least three blogs already but top prize to The Big Yin for calling his piece Welsh Rarebit. For rare it has been over the last few years to see tobacco companies leading from the front.
Yet here it is: Imperial's reply to the Welsh tobacco control consultation. Forest dubs it winner of its Plain English Award, and not without reason: it is clearly set out and structured:
It is also wrong because it attacks the legal market in tobacco:
As The Big Yin points out, Imperial Tobacco is not the first tobacco company to start openly opposing official policy. There is so much to be done, and I hope this kind of document will now surface frequently – my way of saying Up With This Sort Of Thing.
Yet here it is: Imperial's reply to the Welsh tobacco control consultation. Forest dubs it winner of its Plain English Award, and not without reason: it is clearly set out and structured:
- Good –there is a tobacco control policy aimed at reducing youth smoking
- Bad – it has been incompetently conceived and designed
- Ugly – Welsh tobacco policy relies disproportionately on ASH Wales, raising the question whether improper pressure is being applied by 'the anti-smoking lobbying industry'.
It is also wrong because it attacks the legal market in tobacco:
In many communities, where smoking rates are well above the national average, a high proportion of smokers will be sourcing their tobacco from illicit sources and criminal gangs ... Attempts to limit the availability of tobacco from legitimate sources will be undermined by an increase in the supply from organised criminal gangs who will welcome the broadening of the market share.Addressing also civil liberties, property rights and the self-defeating method of denormalisation as a means of persuading adults to give up smoking, this consultation response makes good reading.
As The Big Yin points out, Imperial Tobacco is not the first tobacco company to start openly opposing official policy. There is so much to be done, and I hope this kind of document will now surface frequently – my way of saying Up With This Sort Of Thing.
US Chamber of Commerce and others issue statement opposing plain packaging
Major business interests in Washington have issued an important statement on the implications of Australia's plain packaging policy, and expressed their opposition to this policy.
Although many people appear to feel that the tobacco industry's indignation about plain packaging demonstrates how important plain packaging is in the fight against tobacco, it would appear that the tobacco industry is not alone in its concern for intellectual property in general and the likely benefits to rogue tobacco traders. Two extracts:
The Chamber of Commerce and its allies in this statement have made an important case. Brand protection is a guard against cheap imitation, and health authorities that were really interested in health would not attempt to destroy it. Insofar as it represents an attack on intellectual property, the proposed plain packing measure is a dangerous precedent that threatens the benefits of brand packaging not just for tobacco but for any other line of products. Legality brings with it rights and obligations, and brand protection should not be removed from tobacco – or why did we ever bother with it in the first place?
Although many people appear to feel that the tobacco industry's indignation about plain packaging demonstrates how important plain packaging is in the fight against tobacco, it would appear that the tobacco industry is not alone in its concern for intellectual property in general and the likely benefits to rogue tobacco traders. Two extracts:
However, plain packaging risks establishing a precedent of intellectual property destruction for an entire industry through government mandate that would be very damaging to the legitimate interests of trademark owners to associate their brands with their products, a fundamental protection under trademark lawand:
Moreover, we have genuine concerns that plain packaging will incentivize further the already growing incidence of counterfeit, smuggled and other illicitly traded goods being sold in Australia. There can be little question that plain packaging will make it easier for contraband or counterfeit products to enter the market. This will augment the inevitable downward pressure on prices of legally sold goods when brands are undermined and the market moves toward commoditization. The economic incentives to avoid the legal system will overwhelm any enforcement effort detailed in the legislation. As a country that has supported the Anti-Counterfeiting Trade Agreement (ACTA), Australia should be particularly concerned about these consequences.Simon Chapman, professor of public health at the University of Sydney, tries to explain how plain packaging will indubitably help. I find his logic hard to follow:
Profitability in the tobacco industry today rests largely on high-priced premium brands, which are able to attract higher retail prices purely on the strength of branding and pack image. If all packs will look the same, many smokers will wonder why they should shell out far more for a pack that looks the same as every other brand except for brand name and that internal tobacco industry research shows cannot be distinguished from cheaper brands in blinded smoking experiments. The illusion that premium brands are “better” will evaporate, and much profitability with it.The result of this will surely be falling prices – not an outcome advocated by anti-tobacco activists in general. Chapman is confident that Australia is on top of illicit tobacco, but while it is true that Australia is less exposed than Canada, for example, there is still an issue with illicit tobacco and those involved tend to have an opportunistic streak that would likely be excited by a legitimate-industry-busting initiative like plain packaging.
The Chamber of Commerce and its allies in this statement have made an important case. Brand protection is a guard against cheap imitation, and health authorities that were really interested in health would not attempt to destroy it. Insofar as it represents an attack on intellectual property, the proposed plain packing measure is a dangerous precedent that threatens the benefits of brand packaging not just for tobacco but for any other line of products. Legality brings with it rights and obligations, and brand protection should not be removed from tobacco – or why did we ever bother with it in the first place?
Tuesday, 7 June 2011
Champix off the approved list in France: risks outweigh benefits
They kept this one quiet. (Or have I been asleep for a week?) Hat tip Chris Holmes.
The pill, called Champix in Europe and Chantix in the U.S. but known generically as varenicline, has been tied to everything from violent rages to suicidal thoughts. Reported side effects of Chantix have led to hundreds of lawsuits nationwide, including one filed last month in Pennsylvania following a 2009 murder-suicide.
French health Minister Xavier Bertrand said Tuesday he decided to remove the drug from a list of approved treatments available for reimbursement through his country’s social security funds because of questions about its safety.About bloody time. Well done the French Health Minister. Some recent history is also included in this report:
In another controversy surrounding the drug, the U.S. Food and Drug Administration announced late last week that Pfizer had been asked last year to resubmit thousands of reports on adverse events related to Chantix, a request that came after it was revealed the company had not sent the information through proper channels.
The adverse-event information had been sent as a periodic safety summary rather than as a report required within 15 days for unexpected or fatal events, the FDA said.I could comment but time is short today. Chris has already said what had to be said (comment 5):
Medical authorities the world over CLAIM to have the best interests of patients at heart. They CLAIM to be approaching these problems logically and scientifically.
Therefore it should be standard practice everywhere to try all safe methods FIRST, and only proceed to methods that involve any risk at all if none of the safe methods work. It is an absolute no-brainer. Hypnotherapy, acupuncture and the Allen Carr approach (which is a mild form of hypnotherapy anyway) have all proven themselves to be more effective in the long term than any of the meds, and they all involve NO RISK.
Why are they not being used as a priority to avoid damage to patients? Because of the massive lobbying power of global drug giants and their immoral influence over politicians and medical authorities.
It’s corruption, and it is killing people. Think I’m exaggerating, calling this sort of thing corruption? Check this out: GlaxoSmithKline have just revealed how much cash they lavished on Australian doctors and other medical personnel last year alone: over two million dollars, of which $371,659 was just to go on merry junkets to conferences abroad. In the age of the internet, none of this is necessary but it certainly makes people feel important, doesn’t it? Would YOU like an all-expenses paid trip to Vienna? But that’s nothing: in the same period GSK spent a staggering $96,000,000 on doctors in the USA (link here). Why? Because money talks.
But so do smokers! Spread the word, don’t risk the slimy meds. Even Pfizer can’t force their drugs down your throat. Doctors, I keep telling you: you’ll miss your credibility when it’s finally gone forever. You are signing it away with your own prescriptions pads with dodgy drugs like Champix, every working day of your lives.
BUT HOORAY FOR THE FRENCH HEALTH MINISTER! Monsieur Xavier Bertrand, I salute you! Bravo!He's right. Champix is a drug that is being used to treat something that is far from being universally recognised as a sickness: the desire to give up smoking. And it's not only not the safest option, it's got a known track record (and I don't mean in getting people off tobacco). So let's stop spending our 'health' money on it.
Subscribe to:
Posts (Atom)